Covid-19 recovery and resilience:
what can health and care learn from other disasters?


As Covid-19 swept the globe, countries scrambled to tackle the immediate threat of the virus. Entire new hospitals were built in just days, people have been required to restrict their activities on a scale previously inconceivable during peacetime and a new class of vaccine was developed, trialled and approved within a matter of months. The scale of the emergency response has been extraordinary. But what comes next?
When a disaster, such as an earthquake, a flood or a pandemic, hits emergency plans are quickly enacted and command-and-control structures mobilised. But how to manage recovery isn’t always so clear. How do individuals, communities and countries recover from catastrophic events? How do we know what support is needed, which groups should be prioritised and how should efforts be co-ordinated and managed? And what role should the health and care system play in recovery?
We set out to understand what the health and care system can learn from the experience of recovery from other disasters. While Covid-19 can feel like an entirely unique event, there are parallels with and lessons to be learned from other disasters from the past 20 years. Here we identify key insights from people involved in recovery work around the world. We spoke with people who worked in New Zealand in the aftermath of the Christchurch earthquakes, in New Orleans following Hurricane Katrina, in the wake of the Grenfell Tower fire in London, and many others. Disaster recovery is an under-researched and under-resourced area of emergency planning, but there are plenty of examples to learn from.
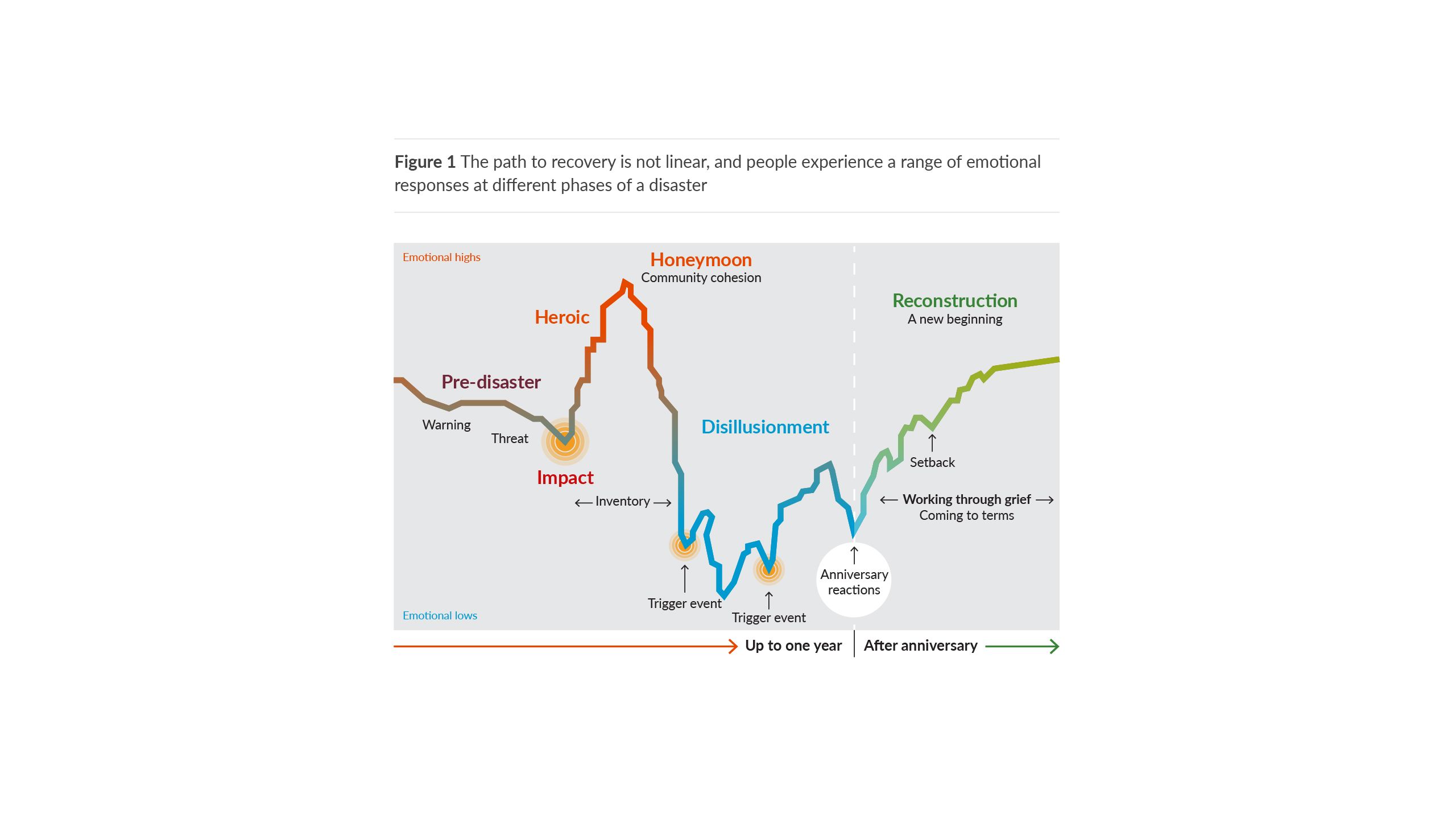
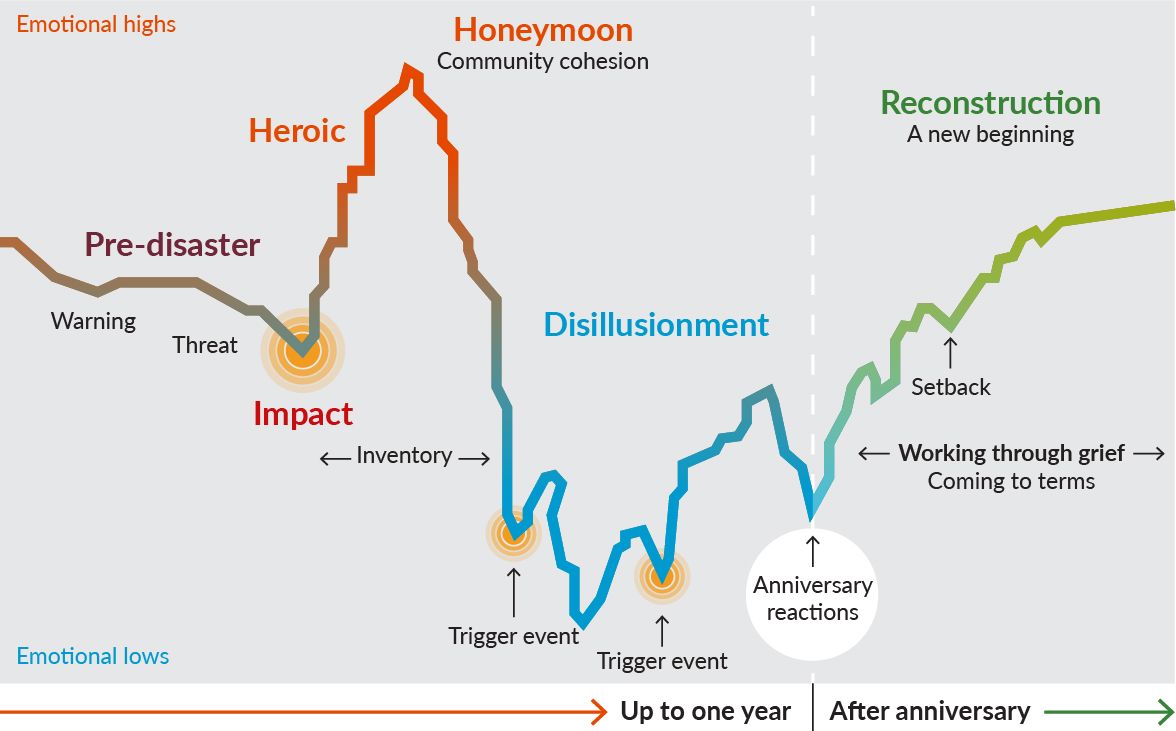
What became clear from our research is that recovery should focus on understanding what individuals and communities need to cope with the impacts of a disaster, and be in a better position to withstand the next one. Know that recovery will be a long haul – start thinking about a 10–15 year timeframe – and know that progress will not be linear (see Figure 1).
In the aftermath of a traumatic event, successful recovery doesn’t just happen. Here we share the four priorities that we learnt require conscious attention and action.



Source: Myers D, Zunin L (2000). ‘Psychological reactions to disaster’ in DeWolfe DJ (ed). Training manual for mental health and human service workers in major disasters, 2nd ed. Washington DC: Federal Emergency Management Agency and Substance Abuse and Mental Health Services Administration. Available at: https://eric.ed.gov/?id=ED459383 (accessed on 24 May 2023).
As Covid-19 swept the globe, countries scrambled to tackle the immediate threat of the virus. Entire new hospitals were built in just days, people have been required to restrict their activities on a scale previously inconceivable during peacetime and a new class of vaccine was developed, trialled and approved within a matter of months. The scale of the emergency response has been extraordinary. But what comes next?
When a disaster, such as an earthquake, a flood or a pandemic, hits emergency plans are quickly enacted and command-and-control structures mobilised. But how to manage recovery isn’t always so clear. How do individuals, communities and countries recover from catastrophic events? How do we know what support is needed, which groups should be prioritised and how should efforts be co-ordinated and managed? And what role should the health and care system play in recovery?
We set out to understand what the health and care system can learn from the experience of recovery from other disasters. While Covid-19 can feel like an entirely unique event, there are parallels with and lessons to be learned from other disasters from the past 20 years. Here we identify key insights from people involved in recovery work around the world. We spoke with people who worked in New Zealand in the aftermath of the Christchurch earthquakes, in New Orleans following Hurricane Katrina, in the wake of the Grenfell Tower fire in London, and many others. Disaster recovery is an under-researched and under-resourced area of emergency planning, but there are plenty of examples to learn from.
What became clear from our research is that recovery should focus on understanding what individuals and communities need to cope with the impacts of a disaster – and be in a better position to withstand the next one. Know that recovery will be a long haul – start thinking about a 10–15 year timeframe – and know that progress will not be linear (see Figure 1).
Figure 1 The path to recovery is not linear, and people experience a range of emotional responses at different phases of a disaster

In the aftermath of a traumatic event, successful recovery doesn’t just happen. Here we share the four priorities that we learnt require conscious attention and action.


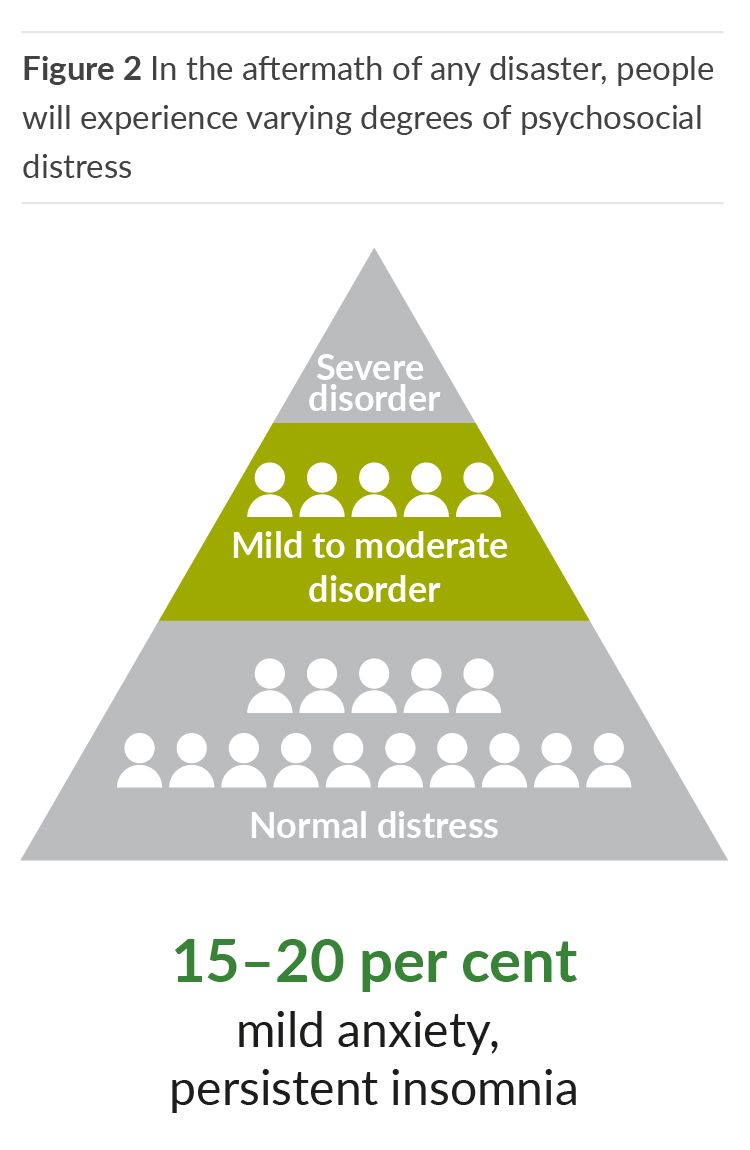
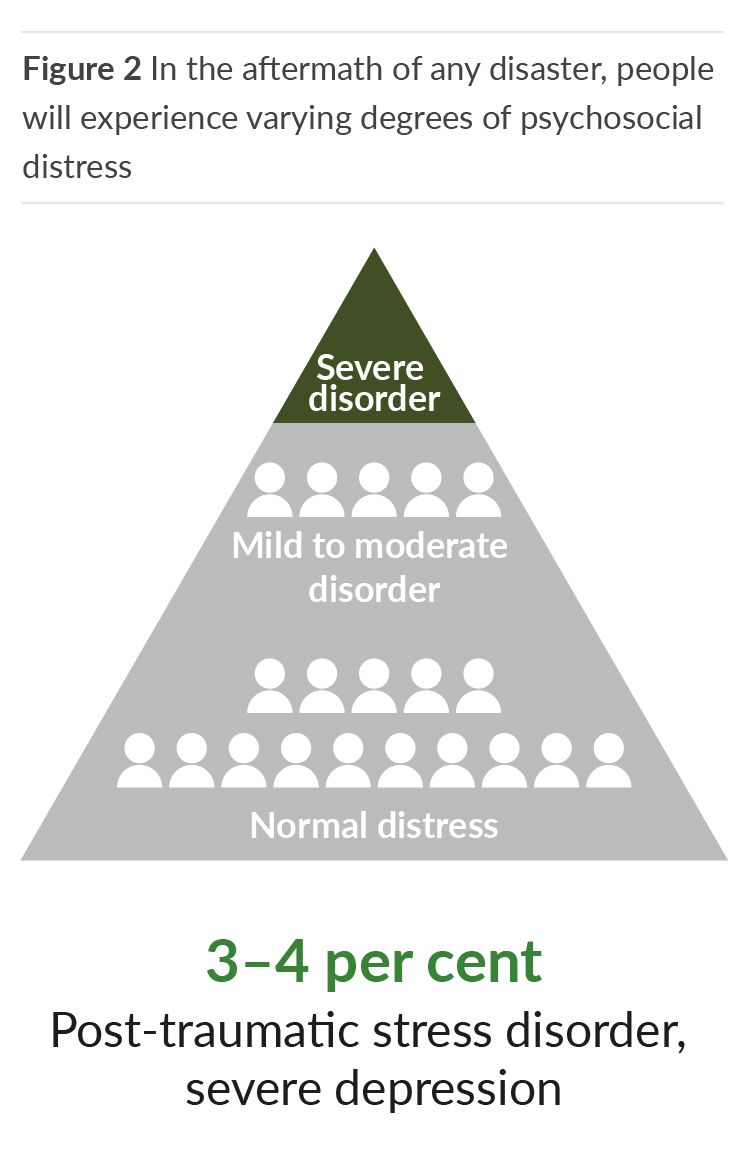
Why is support for mental health and wellbeing essential to successful recovery? In the aftermath of any disaster, large numbers of people will experience some form of psychosocial distress (see Figure 2). For most people, the issues they experience will often be characterised by short-lived anxiety or sleeplessness; an ordinary response to an extraordinary situation and something from which, with the right support, they can recover.
However, during the early months of recovery most will not seek formal help and many will generally not reach the threshold for accessing specialist mental health services, leaving some people at significant risk of not getting the support they need. In the long term, if left unaddressed, these anxieties can escalate into more serious situations requiring specialist support and significantly increase demand for mental health services.
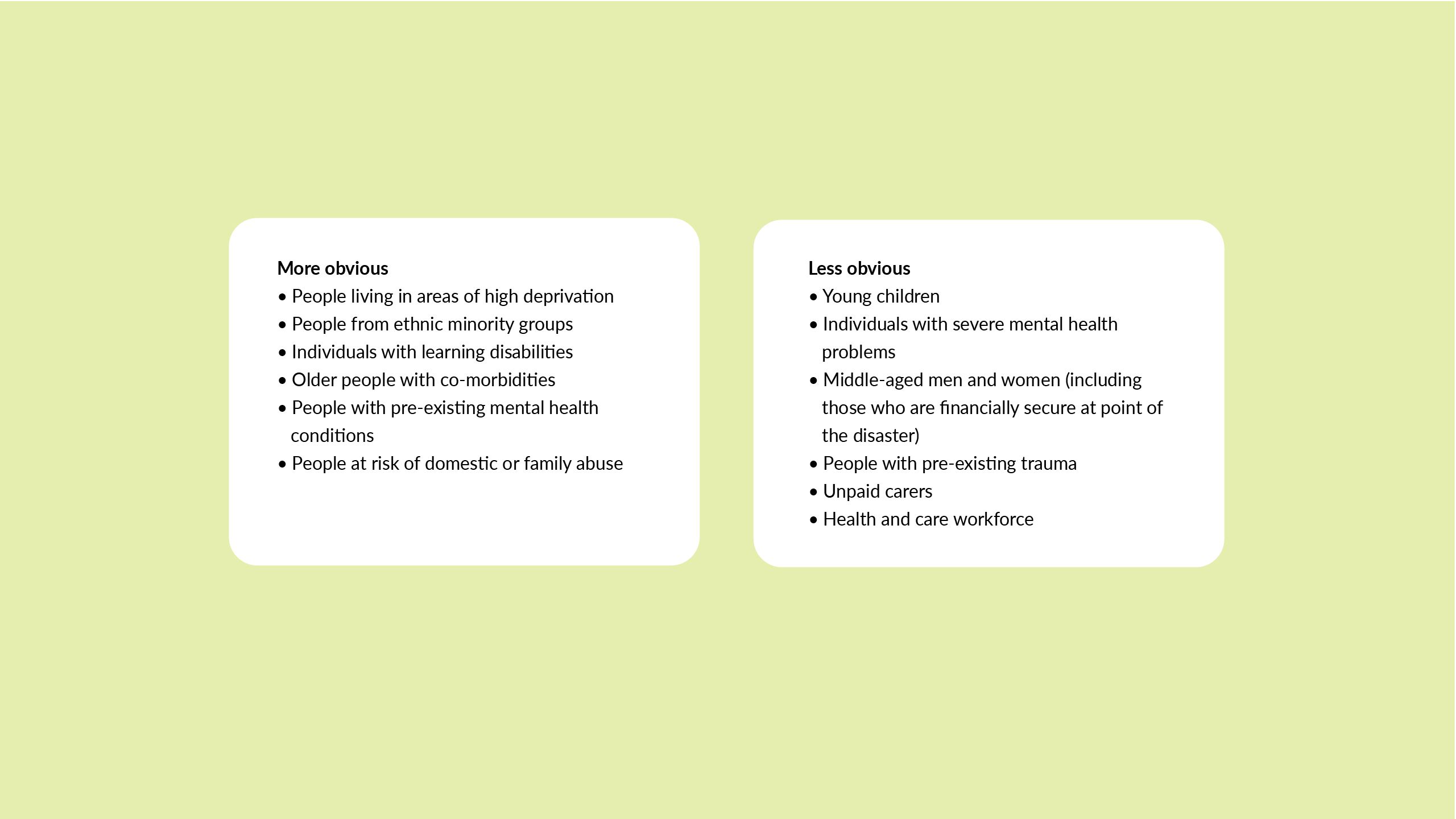
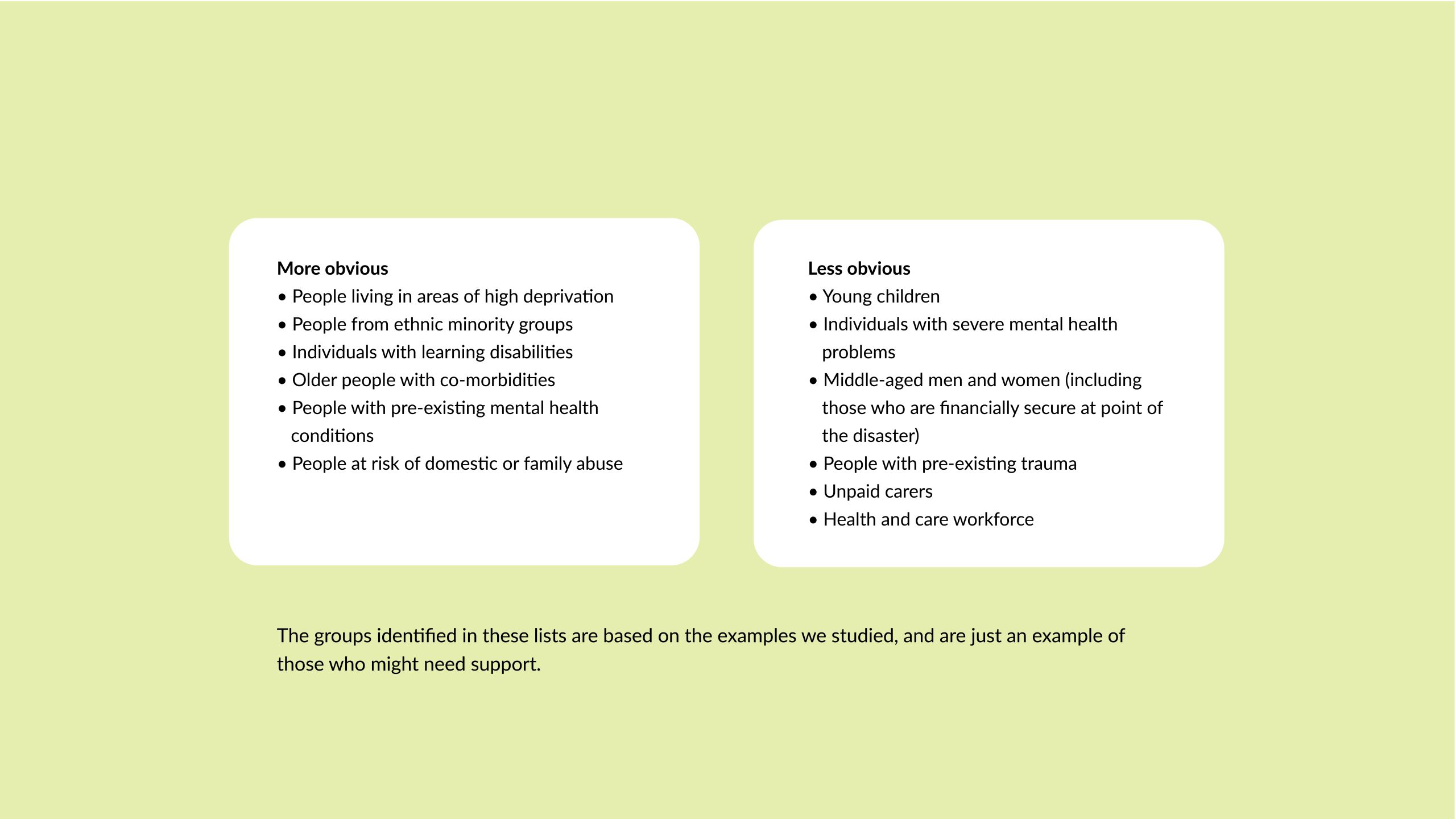
One of the challenges facing community leaders, health care professionals and policy-makers is that it is difficult to safely predict who will be most affected. For most people, the aftermath of any disaster involves living with greater risk and uncertainty. This background level of stress can mean that ‘secondary stressors’ like job or housing insecurity, can push people over the coping threshold.
The impacts of these stressors can be unpredictable; the wider economic impacts of a disaster, for example, may not be experienced for many weeks or months and it can therefore be difficult to identify who might be most at risk. We learnt how middle-aged men (for example following the major rail disaster that destroyed the Canadian town of Lac-Mégantic in 2013 and in New York following the 9/11 attack in 2001), often financially stable at the point of disaster, struggled months later when they lost their job and their house with no financial buffer and no experience of how to access available support. In addition to this, many people may not seek support or even realise that they might need it; especially if everyone around them is experiencing the same symptoms such as drinking too much or sleeping less.
So for recovery to be successful, identifying and assessing the level of community need is essential. Validated psychological tools, like the Sense of Coherence, can offer a helpful framework for measuring psychosocial wellbeing and the impact of interventions on individuals and communities, as well as being a useful predictor of psychosocial health. The Sense of Coherence framework, used after the major rail disaster in Lac-Mégantic, can measure an individual’s capacity to understand, manage, and make meaning in their life. After a disaster it is a way of assessing the degree to which people feel optimistic about the future and the feeling that life is manageable. Those with a higher sense of coherence have been found to be at lower risk of major depression.
We also learnt that children need to be considered in their own right. Not only do they feel the impact of a disaster when it happens, but any stress placed on relationships and normal routines, such as housing, job and financial security will also have an impact on the protective environment offered by a family. Indeed, we heard arguments that children’s psychosocial wellbeing should be viewed as the single most important indicator of success in recovery.



'For recovery to be successful... identifying and assessing the level of community need is essential.'

And once community need has been identified, what then? How are these groups and individuals best supported? While national or regional helplines and campaigns around mental wellbeing – like the All Right? Campaign, established following the earthquakes in Canterbury, New Zealand – can be a helpful way of promoting psychosocial wellbeing on a macro scale, we found that local interventions are critical too. Activities that bring people together in the community can have a positive impact by creating local support that benefits people’s psychosocial wellbeing, without pathologising the difficulties they face. This more informal and more accessible support can have a real impact, as Dr Melanie Irons, who set up an invaluable Facebook group following the 2013 Tasmania bushfires, outlines:
I had psychologists calling me saying, ‘I’ll do free sessions, just let them know…’ And of course, no one did [take up that offer]. But then I had retirees go and take their caravan to someone’s cherry orchard that had completely burnt out and spend a week just helping them get rid of dead cherries…. [They] forged these really lovely friendships, just over very casual, incidental discussions… So, that’s delivery of psychological first aid from community member to community member. I think that’s one of the keys for a quicker and much deeper recovery…
As the experience in Tasmania shows, language is important. Communities affected by disaster often do not see themselves as having mental health needs and individuals can be reluctant to seek help. There can be low uptake of services labelled as ‘psychosocial’ or ‘psychological’ support. In contrast, offering people a chance to share their disaster experience is often met with gratitude and without stigma.
Initiatives that strengthen community connections and provide informal opportunities to share their experiences can therefore play a key role. After the Lac-Mégantic rail disaster, health leaders created opportunities – using outreach workers – for the community to come together and make sense of what had happened. One initiative was to invite people to take pictures of what made them feel proud of their community and people then came together in small groups, so that each person could explain the story behind their picture. ‘[P]eople felt less threatened about talking about their experiences,’ reflected Mélissa Généreux, a Medical Advisor at Public Health Estrie and Associate Professor in the Department of Community Health Sciences at the University of Sherbrooke. ‘Talking about a picture and expressing why you took it – in some way you’re talking about what’s going on in your mind and how you interpret your environment.’ Creating spaces where people could talk about their experiences of the disaster and come together across intergenerational boundaries was a key part of their successful recovery.
These examples highlight how local community groups and grassroots organisations play a critical role in creating and maintaining those human connections that are essential for successful recovery. In the UK, many of these groups will struggle to survive and sustain their impact during Covid-19 and beyond, so infrastructure, funding and support that can anticipate and manage that risk is essential. Recovery can take many years, if not decades, so it’s important to consider how this support will be maintained in the long term.
Finally, we found that having leadership at every level that recognises and prioritises psychosocial support is key. This means putting mental health and wellbeing at the heart of conversations about recovery at a local, regional and national level.


Community resilience is key to the process of recovery, but a community won’t be resilient if parts of it are left behind. It’s already well known that disasters exacerbate existing inequalities. Focusing the recovery effort on communities that experience inequalities can not only aid the process of recovery but, by making communities more resilient, help ensure that they are better placed to cope when the next challenge arises.
So first, what do we mean by ‘community’? There are various lenses that can be applied to help us understand how best to ensure that groups are not forgotten during recovery. Traditional frameworks such as communities of interest (people linked by a shared interest or work); communities of identity (those who have a shared culture or experience); geographical communities (from whole towns to individual streets or tower blocks); and communities of circumstance (people knitted together by a shared experience) all help identify needs of specific groups. However, there are often new groups that emerge during the recovery process that do not fit neatly into this framework – and are not always anticipated or seen to need support. And different parts of the community recover at different times, with some groups more vulnerable to being overlooked than others.




So how can we make sure that all groups get the support they need? Global examples have shown how meaningful community engagement at a local level is as an essential part of successful recovery. This means getting up close and personal with communities to really understand what’s needed and empowering communities to identify those groups who are missing out or struggling themselves. In Christchurch, New Zealand, for example, Maori and Pacifica communities didn’t feel that they’d been appropriately engaged in the re-design of the district health board’s maternity model following the 2010 and 2011 earthquakes, so the health board changed its approach:
We had a number of groups of women who came to our team and said, ‘Great… lovely model but it won’t work…’ So, we then got them all in a room… we gave the women the big thick pens and health sector people had the little thin pens so we could write down too, but what we wrote was nowhere near as obvious as what they wrote. And we ran a session because we said to them, ‘Well, okay, if you don’t think this is going to work, tell us what will.’
Of course, key to engaging meaningfully with communities is the ability to do this in a culturally competent way. The Grenfell Health and Wellbeing service is one organisation that has recognised the importance of developing health care services during recovery that understand and respect the importance of faith, ethnicity, culture and gender. The service is very clear that one size does not fit all.
We already know that the pandemic has had a disproportionate impact on certain groups, including older people and ethnic minority populations, and has exacerbated pre-existing inequalities. Tackling these issues must be a top priority. Alongside this, local leaders must feel that they have the permission and support to focus on the needs of specific groups, as well as the space to innovate and use new methods to address these inequalities in their locality.
In the aftermath of Hurricane Harvey, officials in Texas decided to take a ‘worst first’ approach to tackle deeply entrenched inequalities and prioritise spending on flood protection for communities facing the greatest risk. Instead of using a traditional cost-benefit analysis to determine where funding for flood protection should be spent – a common approach that usually benefits wealthier, white areas where high property values could offer the best return on investment – officials decided to focus funding on more deprived areas with predominantly ethnic minority populations that typically struggled to bounce back after a disaster.
Furthermore, positive and deliberate representation at all levels is an important way of ensuring that groups aren’t left behind. As Marcie Roth, Chief Executive and Executive Director for the World Institute on Disability describes:
Successful recovery… [is when] the people who are actively at that table look like the people in the community… If we’re having a public meeting, we always offer captioning because we know a large number of people are going to benefit, so that’s just a standard… Our budget and our processes very clearly say that we’re serious about engaging the whole community in the recovery process…. [S]ome of successful recovery is just using language that intentionally demonstrates inclusion and some of it is in very intentionally taking actions that are not just to placate some people or do it because the law requires it, but because the community has learned that the community is more resilient. That the community is better for having committed to this.


The most successful examples of recovery put a conscious focus on collaboration across agencies, organisations and services. And while ‘collaboration’ might be an increasingly familiar concept to the NHS, for recovery it needs to go beyond joining up services and consider how greater community resilience can be built.
National and local health services, local authorities, voluntary sector organisations and community groups all bring different perspectives that help ensure that the needs of the local community are genuinely heard and acted on. Community groups in particular bring vital insights and connections that should be central to planning and delivering recovery programmes, alongside local government which has significant experience in community engagement and public health. By working with the right people, you can get a richer understanding of the issues people face, have greater legitimacy in determining priorities for recovery and ultimately provide support that will be more likely to make a difference. And working in this way can not only help recovery from one disaster, it also helps to build resilience to future disasters as the networks are already in place, with real connections to the communities they serve.
But effective collaboration can be tricky and doesn’t happen naturally. At the best of times, managing groups with different expertise and cultures and re-evaluating what’s needed over time is complex, with leadership and accountability not always clear. And when those doing the work have also experienced the disaster themselves, the work becomes even harder.
Following the earthquakes in Canterbury, New Zealand, in 2010 and 2011, and the devastating aftershocks that continued to have an impact on the community, it was an organogram (jokingly named the ‘horrendogram’) showing all the organisations involved in recovery that helped local leaders come together and identify what work needed to be done and who needed to be involved – and how that might change over time. For example, to support children’s psychosocial wellbeing, the local health board worked with leaders from social care, education and local government. The group met regularly and built a shared understanding of what good would look like for them. When a mosque was attacked in Christchurch years later, local leaders had already learnt how to bring people together, which allowed them to work at pace to respond to this latest disaster, as Carolyn Gullery, former Executive Director of Planning, Funding and Analytics at Canterbury District Health Board, told us:
Health and education spent the weekend designing our response so that on Monday, when the kids turned up at school, the teachers were all equipped to know exactly how they needed to work with the class… So, that’s what happens… when people get used to working together and that’s the great thing about a crisis… we instinctively pull together to do stuff like that. How many central bureaucracies do you know who could redesign an education programme between Friday and Monday?
'By working with the right people, you can get a richer understanding of the issues people face... and ultimately provide support that will be more likely to make a difference.'
For David Wales, a customer experience consultant based in the UK with experience in the fire service and international disaster recovery, it’s about ‘moving away from a collection of 12 people representing their organisations and their career aspirations… to a group of people saying we've got a common purpose, I think I can help this way. ’ He told us:
You cannot have an effective multi-agency organisation that has not discussed, at least in principle, some of those ethical and moral issues about what do we value, how do we see our purpose. Because actually if you do that bit, and that's clear and explicit, transparent and very, very visible to you, decision-making's a lot easier.
Once these groups focused on recovery have been established, the next task is to understand the kind of support that people need and want, what David refers to as ‘the customer experience’. But this too requires conscious action. Removing barriers to engagement – this might be providing transportation or offering signing at planning meetings – and making proactive contact with individuals and communities can help to make sure collaboration is truly representative.
This can be supported by working with ‘connectors’ – people and organisations in the community who are trusted and respected. Who these people are will vary across communities. In the Philippines following Typhoon Haiyan, the Catholic Church played a key role in sharing messages between those who needed support and those delivering it; in Tasmania, Australia, after the bushfires, it was Dr Melanie Irons who played this central role after creating a popular community Facebook group. Closer to home, Fatima Elguenuni works as a community consultant for Central and North West London Mental Health Trust. A local resident and former NHS employee, she worked to build trust between the local community and the NHS and local authority in the aftermath of the Grenfell tragedy. One early step was to explain to the system why a visit to the tower would help survivors and bereaved relatives. Securing this visit helped people to feel that their needs had been listened to.
Long-term investment is key for voluntary and community organisations to be able to support communities beyond the initial response. For Jane South, Professor of Healthy Communities at Leeds Beckett University, it’s not just supporting individual organisations but also making sure the infrastructure is in place: ‘which probably means funding and other types of investment into the voluntary sector organisations, especially some of the umbrella bodies that have local networks’.
Ensuring these organisations and individuals can continue to work and develop relationships will support recovery efforts and build community resilience for the future.












Underpinning much of the recovery work are those working in health and care themselves. We already know the toll Covid-19 is having on the health and care workforce, with rising demand and shortages of protective equipment leading to increasing stress, exhaustion and burnout.
Evidence from disasters across the world shows that, in addition to managing the initial burden, people who work in health and care are also at an increased risk of developing mental health problems following disasters, such as post-traumatic stress disorder (PTSD), depression, anxiety and compassion fatigue. In Fukushima, Japan, following the earthquake in 2011 this culminated in high levels of absenteeism among health care workers for up to 18 months after the disaster, with nurses experiencing significantly greater stress levels than the general population four years after the disaster. If the health and care workforce is to support communities through recovery, it needs to be recognised and supported as a community with its own needs.
In Christchurch, New Zealand, health leaders understood the connection between the health and care workforce and the community. The local health board continued to support and develop community-based health and care services, despite much of the physical infrastructure being destroyed by the earthquakes. Carolyn told us:
There were two reasons for doing it. One was to make sure that we didn’t get workforce flight… But secondly, it sent a really strong signal to our community that everything else may be going to hell but your health system is okay. They are still there. They are still delivering services every day. You know, your GP is still there.
So, what strategies or actions could help health and care staff recover and build resilience in teams?
Leading in disaster recovery, a pocket book of wisdom from more than 100 recovery leaders, makes one thing clear: usual methods of support for staff are not enough – more is needed.
Your team not only provides support to disaster-impacted people but are also likely to be impacted themselves. Understand the load they carry, how long they will carry it for and work with them to make it manageable. Even the most capable and resilient people need support.
Staff need to be given the time, space and resources to recover, which might include adequate breaks and time off following intense periods, a supportive work environment, access to training and education programmes and access to psychological support. In New York following the 9/11 attacks, Project Liberty sought to overcome the stigma around mental health support with a media campaign and free counselling service, with the slogan ‘even heroes need to talk’.
Leaders at all levels need to recognise the importance and value of supporting the workforce and to consider their role in in helping this group to recover from such a significant and prolonged event. Evidence suggests that all health and care staff are at risk, regardless of the roles they took on during the pandemic. For example, following the SARS outbreak, staff who had been in contact with SARS patients were more likely to experience PTSD, as might be expected. However, further research has shown that health care staff as a whole – irrespective of their contact with SARS patients – experienced more psychological problems than the general population. It’s not hard to imagine a similar response to Covid-19, given the disruption to people’s work, the perceived risk of infecting family members, and the disproportionate impact of Covid-19 on the health care workforce. Just like the wider population, it’s not easy to predict exactly who will need help.
Throughout the pandemic health and care staff have often been referred to as heroes, but this image shouldn’t mask the reality of their experience. Many of the challenges facing the workforce are longstanding but have been exacerbated by the pandemic. Leaders should use this time to make wellbeing a priority, especially when under great pressure to deliver services at pace and ‘get back to normal’. Longer term cultural change is needed to ensure collaborative, compassionate and inclusive working environments, with leaders at all levels tackling workload issues and leading cultural change to support them to provide the care they want to provide.


At a time when attention is still on the response to the pandemic, it is hard to focus on what comes next. In the face of growing patient need, the focus will inevitably be on getting services back up and running, and tackling the backlog of treatment. But this alone will not be enough to recover from the impact of the virus. We have learnt that a focus on ‘community recovery’ – or rather ‘community-led recovery’ – is essential.
We learnt that it takes great courage, stamina and empathy to skilfully work out together what successful recovery looks like. For many, that will challenge ideas of who leads and how decisions are made. It is likely to be exhausting and rewarding. Thinking about what comes next is daunting especially when people are still reeling from the impact of the virus. By investing in the resilience of communities and supporting community-led approaches, a successful and sustainable recovery is within our grasp, with individuals and communities in the best possible health to cope with what comes next.
Unfortunately, there are multiple disasters that provide valuable lessons for recovery. In particular, we drew on the following disasters for this research:
- the Canterbury earthquakes, including thousands of subsequent aftershocks, took place in New Zealand in 2010 and 2011
Hurricane Katrina, which made landfall in New Orleans and the surrounding area in 2005 - Storm Sandy, including the storm surge that hit New York City in 2012
- Storm Desmond and the Cumbrian Floods of 2015
- the Manchester Arena bombing in 2017
- the Grenfell Tower Fire in 2017
- the World Trade Centre attack, New York, September 2011
- the Fukushima Daiichi nuclear accident caused by the Tōhoku earthquake and tsunami in Japan in 2011
- The severe acute respiratory syndrome (SARS) outbreak in 2003
the Lac-Megantic rail disaster that resulted in a fire and explosion in Quebec, Canada in 2013 - Typhoon Haiyan, known in the Philippines as Super Typhoon Yolanda, which made landfall in the Philippines in November 2013
- Australian bushfires, including the Black Saturday Bushfires in Victoria in 2009, the Tasmanian bushfires in 2013, and the fires in New South Wales in 2019.
Credits
Thank you to all the people from across the globe who were interviewed for this piece and who generously shared their experiences and insights with us.
Project team Julia Cream, Alex Baylis, Joni Jabbal, Gbemi Babalola, Siva Anandaciva, Megan Price, Helen Joubert, Andrew McCracken, Clare Sutherland, Deena Maggs and Sarah Murphy.
Published 4 February 2021
This work builds on research undertaken during the first wave of the Covid-19 response and funded by the NIHR Policy Research Programme, as part of the Partnership for Responsive Policy Analysis and Research (PREPARE), a collaboration between the University of York and The King’s Fund for fast-response analysis and review to inform the Department of Health and Social Care’s policy development. The information included here was independently researched, developed and written by The King's Fund.
We've been supporting health and care leaders throughout the Covid-19 pandemic by offering a range of resources and practical guidance.
>> Take a look at the latest resources in our Leading through Covid-19 series.
